From the early 18th century, the medical concept of rhythm changed mainly for two reasons: the first was the Mechanistic perspective that was slowly penetrating medicine; the second was the use of new portable timing devices that brought more accuracy to observation. These new circumstances allowed the generalization of the concept of beat, its later transformation into that of wave, and their association with the concepts of frequency and regularity or periodicity, which was now taken in a new sense freed from its astrological connotations.
Rating the Pulse – Rhythm as Beat (from Floyer to Stokes – 1707-1878)
In the 17th century, timing devices made spectacular progress. At the end of his life, around 1637, Galileo Galilei dictated to his son the plans for one of the first clock using a pendulum. Probably based on Galileo’s idea, Christiaan Huygens created the first pendulum clock in 1656. Then, clockmakers’ realization that only pendulums with small swings of a few degrees are isochronous motivated the invention of the anchor escapement around 1670, which increased further the accuracy of the clocks. The seconds pendulum—also called the Royal pendulum—0.994 m (39.1 in) long, in which each swing takes one second, became widely used in quality clocks after 1680. The increased precision resulting from these developments caused the minute hand, previously rare, to be added to clock faces beginning around 1690.
This new instrument, which was much more precise than previous time devices was to radically change the conditions of scientific experiment in astronomy and physics but also in physiology and medicine. It was not the only cause but it strongly participated in the shift from pulse rhythm as ratio of time-lengths to pulse rhythm as beat, frequency, and regularity.
Townsend has described how “the medical literature of the 18th century is replete with pulse numerations” (Townsend, 1967). One of the first of a long series of physicians who emphasized the importance of rating the pulse was Sir John Floyer, who published The Physician’s Pulse-Watch in 1707, and had a special “pulse-watch made, which ran 60 seconds,” to that aim. Although his watch was running too fast, he made numerous observations with it, noting the effects of age, sex, meals and exercise, and, remarkably, calculating the effect of variations in age, which was reviving some of the most fruitful intuitions of Herophilus (Fleming, 1997, p. 18).
After Floyer’s introduction of the modern pulse count, physicians started to record their observations in their daily practice based on the number of pulse beats per minute. Bryan Robinson (1680-1754), an Irish physician, studied the pulse rate in different times during a day, and in people with different heights (1732). Jean-Baptiste Senac (1693-1770), physician to Louis XV, after studying one hundred soldiers, six feet in height, reported that the normal pulse rate ranged from 60 to 90 beats per minute. Other observations were also made such as the pulse rate to increase with age. In Observations Respecting the Pulse (1796), William Falconer (1744-1824) made numerous tables by which the degree of fever might be determined based on the proportion of the accelerated to the normal pulse (Ghasemzadeh & Zafari, 2011, p. 5).
By the mid-19th century, thanks to the French Pierre-Charles Alexandre Louis (1787-1872), and the Irish Robert James Graves (1796-1853) and William Stokes (1804-1878), rating the pulse had become part of routine clinical practice in Europe (Fleming, 1997, p. 19).
In the 19th century, the “pulse” itself retained most of its old sophisticated qualitative connotations, but due to the improvement of portable timing devices and the spreading of pulse rating practices, the concept of “rhythm” which was associated to it surreptitiously changed: it began to mean first frequency and regularity and only secondarily ratio.
This shift was recorded in the French Dictionnaire des sciences médicales (1820). In the article “Pouls,” its author, Serrurier, differentiated first between the “strength and intensity of each pulsation” and the rhythm strikingly defined as “mode of the pulsations.”
The pulse, in the natural state, is equally soft, supple, free, not frequent, not slow, vigorous, without seeming to make any sort of effort. But because of the countless differences which nature presents, in the various diseases, with respect to the regularity of the pulse, we can reduce them, according to M. Double, to two general points of view which cover all nuances and modifications.
The strength or intensity of the pulsations.
The rhythm or mode of these pulsations.
In the first case, the modifications derive from each of the pulsations considered in isolation.
In the second case, they emerge from the comparison of the pulsations between them, and in a given time. (Dictionnaire des sciences médicales, “Pouls,” 1820, p. 443, my trans.)
A few pages below, Serrurier completed the definition. The “mode of the pulsations” itself comprised “frequency,” i.e. number of beats per minute, and “regularity,” in which he included regularity in time, but also in strength and speed.
The observations concerning the change of the pulse rhythm in the affections which we have just pointed out demonstrate the value of the two general points of view which we must always have in mind in all diseases of the organs: the strength or intensity of the pulsations, and the rhythm or mode of these pulsations. By considering each of these pulsations in isolation, we can guess from where their modifications can derive, and we assure our diagnosis; likewise, by comparing the pulsations between them, and in a given time, we can establish, according to their frequency, their regularity and their irregularity, their strength or their weakness, their vivacity or their slowness, a prognosis all the more true that we make coincide the signs drawn from the pulse with those exhibited by the whole sick individual. (Dictionnaire des sciences médicales, “Pouls,” 1820, p. 445-446, my trans.)
Two decades later, the Belgian Répertoire général des sciences médicales au XIXe siècle (1843) was even more concise. Normal rhythm, although still defined as ratio, included only two aspects: regularity and frequency.
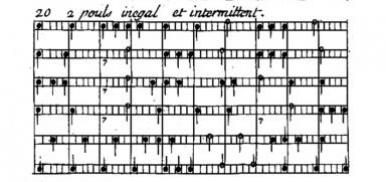
2. Sorts of pulse defined according to the characters of the rhythm. These sorts of pulse, based on the succession or the ratio of the pulsations between them, present sometimes regular beats and sometimes irregular beats [tantôt des battements réguliers et tantôt des battements irréguliers]. We include into the first division the more or less frequent pulse, and into the second the unequal and intermittent pulse. Those are the characters of the pulse that are the easiest to notice. (Répertoire général des sciences médicales au XIXe siècle, “Pouls,” 1843, p. 332)
Timing the Pulse – Rhythm as Beat (Marquet – 1747)
In 1747 François-Nicolas Marquet (1687-1759) published a Nouvelle Méthode facile et curieuse pour apprendre par les notes de musique à connaître le Pouls de l’Homme, & les différens changemens qui lui arrivent, depuis la naissance jusqu’à la Mort – An Easy and Curious New Method of Knowing by Musical Notes the Pulse of the Man, & the Various Transformations which Occur from Birth to Death. A second edition was published in 1769 (this the one I used; on Marquet see, Dos Santos Costa, 2008; Pesic, 2016; Pennuto, 2017).
As Struthius and Mercado two centuries before, Marquet followed Galen on many points while proposing to use the musical notation to help the physician during his visits to note and classify the different varieties of pulse. But in the meantime, both physiology and theory of music had changed.
Like his predecessors, Marquet was fond of Galenic concepts. Although he rejected some of the most bizarre pulses, he recognized the pulsus dicrotus or double, caprizans, vermicans and formicans, the deep or superficial pulses. To those, he associated explanations relating pulse irregularities to excess of sulfur, salt or serum, which very soon excited the irony of Menuret de Chambaud, the author of the article “Pouls” in Diderot’s and d’Alembert’s Encyclopédie.
The abundant sulphurous part produces a great and vehement pulse, the saline an intermittent pulse, the serous a small, weak, and late pulse, the globulous a frequent pulse. And when these causes are united and act together on the pulse, they result in this kind of pulse that is called convulsive. The intercadent, escaped or intermittent pulse owes its origin to air bubbles which enter the blood, and which make, in the places where they are, the dilation of the artery imperceptible; from that, one may judge of the author’s ideas, genius, and light. (Menuret de Chambaud, “Pouls,” Encyclopédie, 1756)
But his approach was, at the same time, deeply influenced by the modern spirit of precision and quantification. What he presented as a “facile et curieuse” method was actually inspired by a strong concern for updating the qualitative technique of the ancient pulse lore and making it meet the modern mechanistic standard.
Marquet defined the pulse according to the ultimate Harveyan physiology. The pulse felt by the physician on the wrist of his patient was “a beating of the heart and arteries” which made the blood circulate “from the center to the circumference and from the circumference to the center.”
The pulse is a beating [le pouls est un battement] of the heart and arteries, which makes the blood flow from the center to the circumference and from the circumference to the center. The first movement that occurs in the heart of the fetus produces the beat [le battement], which continues until death. (Nouvelle méthode..., 1747-1769, p. 9-10, my trans.)
In his introduction, Marquet explained that this beat was the result of “alternative” motions of the heart and arteries but he still believed, as indeed Harvey, that the beats that were felt by the physician were simultaneous.
The beating of the heart [le battement du cœur] and the arteries is alternative [alternatif], it is called systole and diastole; the systole is the contraction of the heart and arteries, and the diastole their dilatation. At the same time that the heart contracts, the arteries dilate to receive the blood, and carry it to the extremities of the body, where it is then to be carried to the heart through the veins. [...] Therefore, one must feel the beating of the heart and arteries, at the same time. (Nouvelle méthode..., 1747-1769, p. 10-12, my trans.)
Marquet used a hydraulic metaphor, comparing the human body to a “hydraulic machine,” but surprisingly he did not present the heart as a pump but held it instead similar to “the pendulum in a watch, or in a clock.” The heart was like a timing device and therefore the pulse like a regular beat.
The heart holds the same rank and performs the same functions in man, as the pendulum in a watch, or in a clock; the veins and arteries serves as wheels and the nerves are the ropes which make the hydraulic machine act. (Nouvelle méthode..., 1747-1769, p. 1, my trans.)
Marquet retained the old Galenic concept of “eurhythm” but he changed greatly its definition as much as those of its various deviations. Whereas the Pneumatics and Galen in Antiquity, as well as Struthius and Mercado in the 16th century, differentiated between “eurhythm,” “pararhythm,” “heterorhythm,” “echrhythm,” and “arhythmia” according to a series of age groups which were respectively characterized by a typical ratio—1/1; 2/1; 2/2; 1/2 or ½/½; 1/1; 2/2; 4/4—he proposed to classify them according to three criteria which were based on a very different logic: regularity, frequency and degree of complexity.
Health depended on a well “regulated” functioning of the human machine; illnesses occurred when the machine was deregulated.
So long the movement of the heart and the arteries is regulated [est réglé], the human body remains in perfect health, but as soon as this movement is disturbed by some accident, the health is altered by an infinity of diseases. (Nouvelle méthode..., 1747-1769, p. 1-2, my trans.)
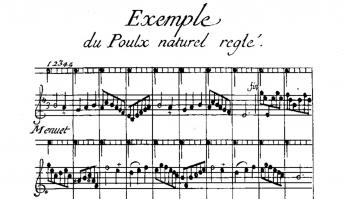
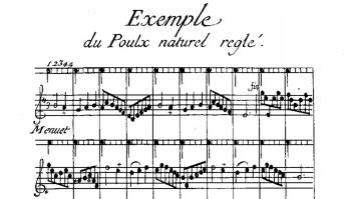
Whereas for Struthius the “natural rhythm,” which served as benchmark for measuring the deviation of the pulse, was the “equal rhythm” characterized by a n/n ratio, it was now qualified as “natural, regulated and tempered pulse” and defined first by its regularity—all the pulsations were supposed to have the same strength, the same cadence, and the same interval of five times that “one notices between two pulsations or from a beat to the next”—and also by its number of beats per minute—as for Kepler and probably for the same astrological reason, it was supposed to beat sixty times in a minute (p. 32). Marquet did not provide more explanation for this particular number. Strangely enough, given that the pulse comprised five times, the natural pulse usually emulated the tempo of a minuet, or a dance in ³/₄ time signature, that was to be sung or remembered while one took the pulse.
The natural, regulated and tempered pulse [Le pouls naturel, réglé et tempéré] is one which has the same force, the same cadence [cadence], or the same interval, and which has five times [cinq temps] between each beat or pulsation [entre chaque battement ou pulsation]. It is usually similar to the cadence of the minuet in movement [la cadence du menuet en mouvement], it also imitates the second of a well adjusted/regulated clock [une pendule bien réglée]. When it is calm and temperate, it is about sixty pulsations [soixante cadences] or so, and runs sixty minuet cadences [parcourt soixante cadences de menuet] in a minute, and 3600 in the lapse of an hour. (Nouvelle méthode..., 1747-1769, p. 34-35, my trans.)
Naturally, as a good Galenist, Marquet recognized that some people, depending on their specific temperament, their gender or their age, had a different natural pulse, but the only significant difference he mentioned was that the latter run faster or slower.
There are nevertheless certain individuals endowed with a lively and bilious temperament, whose pulse, though natural, increases in speed by one degree, or one time in each pulsation [dans chaque pulsation]; others, on the contrary, of a phlegmatic or melancholic temperament, whose blood is so thick and its circulation so slow, that one can count, especially in the morning, up to six times between each beat [jusqu’à six temps entre chaque battement]. (Nouvelle méthode..., 1747-1769, p. 35-36, my trans.)
The pulse that deviated from this norm “by strength or movement and often by both” was “unnatural” and could vary in many ways (p. 40). These differences could be “simple or composite.” The simple pulse was divided into “great and small, equal or unequal, deep or superficial, hard or soft, etc.”; the composite pulse instead could be “subdivided ad infinitum” (p. 41). All in all, Marquet counted no less than twenty-four different kinds of pulse, classified by their degree of complexity and presented with each corresponding pathophysiology.
To legitimate the use of musical notation to describe and assess these different pulses, Marquet referred, as expected, to the traditional authorities of Avicenna, Savonarola, Saxon, Fernel, and naturally Herophilus—he did not mention Struthius nor Mercado (p. 4-5). But his own argumentation was based on the modern concern for precise quantification. Marquet compared his use of musical notation to the two main scientific analytical systems: the series of numbers and that of letters. Notes were mere equivalents of numbers and letters.
There is not more oddness in describing [peindre] the pulse with notes than in describing [peindre] the sounds of music with the very same notes; numbers with figures [les nombres avec les chiffres]; and finally, words with the letters of the alphabet. (Nouvelle méthode..., 1747-1769, p. 4, my trans.)
Moreover, since Struthius’ and Mercado’s time, the theory of music and the notation had changed. The ancient mensural notation system, which had been used for European vocal polyphonic music from the later part of the 13th century until about 1600, had been replaced by the modern notation system, which now featured clef, time signature and bars or measures, and little by little directions for tempo and dynamics. This new system provided a tool for timing music associating versatility and precision thanks to its remarkable capacity to accurately record the continuous changes in the duration of notes within the reliable time frame provided by the regular succession of bars or measures.
It is necessary that the one who wants to learn these principles have at least some superficial knowledge of music, so that, by beating the regulated measure [battant la mesure réglée], he gets used to know the right cadence of the pulse [la juste cadence du pouls] by comparing it to that of the music. (Nouvelle méthode..., 1747-1769, p. 33-34, my trans.)
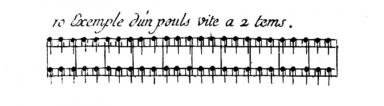
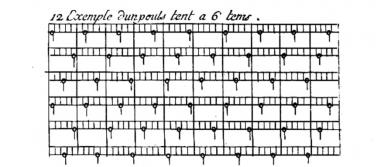
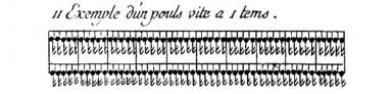
The “natural” pulse—that which was “regulated and temperate”—was noted by quarter notes placed between two parallel lines, and which were separated by five small vertical lines that represented the five times between two successive pulsations. Every pulsation, i.e. every quarter note, was placed next to a vertical larger line that corresponded to each bar or measure of the minuet which was noted below.
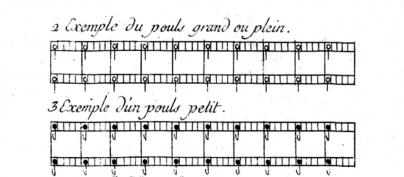
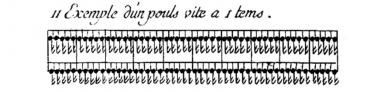
The other durations of each pulsation were noted accordingly: the great or full pulsation, frequent in pleurisy, pneumonia and hemorrhage, with half notes; the small pulsation frequent in weakness, cachexia, slow fever, with eighth notes; and the vermicular pulsation, frequent in fatal disease, with sixteenth notes (p. 30-31 – see table n° 11).
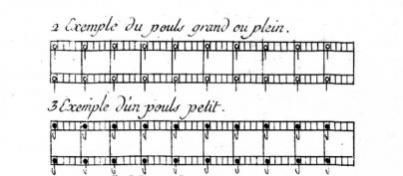
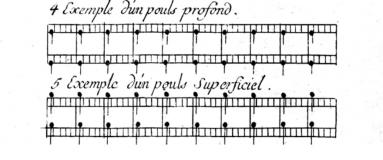
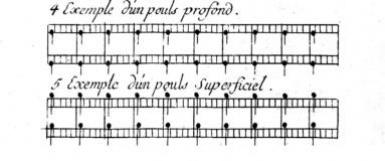
Marquet noted also the volume and strength of the pulse with the location of the notes on the staff : if the note was placed below the first line, the pulse was said to be concentrated; on the first line, it was said deep; between the two lines, it was natural; on the second line it was high and above the second line it was superficial.
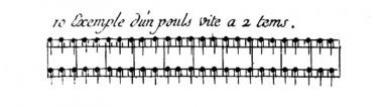
The frequency was noted by a greater or lesser number of times between each pulsation, for instance 2 times for a fast pulse and 6 times for a slow pulse.
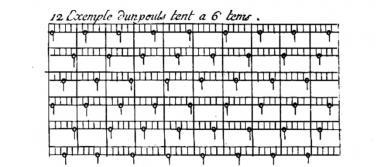
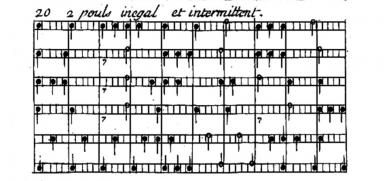
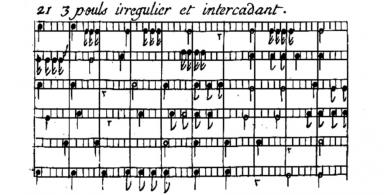
Finally, in addition to the duration, the strength, and the frequency of the beat, Marquet noted its regularity and order according to a scale of growing complexity. If the note was on the first time of the measure, the pulse was normal. If instead it was noted on another of the five spaces representing the pulse times, the pulse was “irregular or unequal in movement.”
If we count more or less of these spaces between each beat [entre chaque battement], the pulse will be irregular or unequal in movement [irrégulier ou inégal en mouvement]; if the note is not placed between the two parallel lines, it will be unnatural in its strength. (Nouvelle méthode..., 1747-1769, p. 32, my trans.)
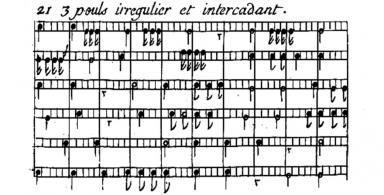
One just have to look at the scores representing the goat-like pulse (caprisant) and the convulsive pulse to realize how precise this method was.

Thanks to this system, Marquet could note both the variation in strength, duration, frequency of one pulsation, and the frequency, regularity and order of a series of pulsations. The only important measure he did not provide, except by referring to the physician’s memory of a well known dance, was the tempo that allowed to measure the frequency, which was not fixed in the 18th century. In his famous book, On Playing the Flute (1752), Quantz himself relied on “the pulse beat at the hand of a healthy person [...] approximately 80 beats per minute” as his time standard. Along with Galileo and Kepler who measured observation time with their own pulse, Quantz used the pulse, not a clock, to prescribe tempi (Pesic, 2013, p. 1).
In the last two examples that were given—the “goat-like” and the “convulsive” pulses (fig. n° 22 and 23)—it became clear that the pulse rhythm was not any longer composed of simple ratios between dilation and contraction of the arteries but of all these measures concerning the pulsations (i.e. only the dilations) either alone and/or observed in series. Although it still was a discrete system of notation, Marquet anticipated, without any mechanical instrument, the oscillating graphs that were to become common in the 19th century.
Feeling and Hearing the Pulse – Rhythm as Sign (from Solano to Laennec– 1731-1819)
During the 18th century, quantitative and qualitative diagnosis methods remained firmly at odds with each other. Physicians fond of Mechanism and mathematical measure rejected the old Galenic pulse lore that was, in their opinion, too long and difficult to learn, too complicated to implement, and that could only deliver vague guesses for diagnosis as much as prognosis. In 1772, for instance, William Heberden (1710-1801) declared that “such minute distinctions of the several pulses exist chiefly in the imagination of the makers” (quoted by Fleming, 1997, p. 21). These physicians substituted humoral view, qualitative observation, and, as far as rhythm was concerned, ratio between dilation and contraction, with an overall mechanistic perspective, quantification, and frequency of the pulse beat.
But others, who according to Menuret’s testimony were a small if active minority, rejected the Mechanistic view on behalf either of a new version of the old humoral physiopathology or of a more recent Vitalism. These physicians thought that the Galenic pulse lore was still of great help to medicine, although it had to be deeply renovated. All of them supported qualitative observation, and paid great attention to the various aspects of the pulse rhythm that were considered as signs to be interpreted.
This reaction against Mechanism began with a Spaniard, Francisco Solano de Luque, nicknamed “el pulsista” (1684-1738). In his Lapis Lydos Appollinis. Methodo segura y mas util asi para conocer como para curar las enfermedades agudas – The Touchstone of Appolo. Secure and Most Useful Method to Know How to Cure the Acute Diseases and his Observaciones sobre el pulso, published respectively in 1731 and 1787, Solano revived the ancient doctrine of the critical pulse. The meticulous observation and interpretation of the pulse could help the physician, Solano claimed, to determine the course of the disease and especially the moments of crisis which could be fatal or, on the contrary, bring relief to the patient by triggering the critical excreting of morbid humors.
A few years later, James Nihell, an Irish physician practicing in Spain, became interested in Solano’s teaching on crisis and pulse rhythm. He popularized it in 1741 in his own Nuevas y raras observaciones, para prognosticar las crises por el pulso sin alguna dependencia de las señales criticas de los antiguos – New and Extraordinary Observations Concerning the Prediction of Various Crisis by the Pulse.
Nihell’s treatise on the pulse was followed by several others, which drew on Solano and Nihell, for example in 1753 by Malcolm Flemyng (ca. 1700-1764): A physiological comment on Solano’s prognostics from the pulse, and in 1758 by Daniel Cox (dates unknown): Observations on the intermitting pulse, as prognosticating, in acute diseases, according to Dr. Solano, a critical diarrhoea – or, as indicating the use of purging remedies, which had height editions in English and seventeen in French between 1760 and 1785 (cf. worldcat.org).
These attempts at defending, until late in the 18th century, the old humoral physiopathology and the Galenic pulse lore, was certainly quite reactionary from a medical viewpoint, but it must also be related with the development of the modern theory of semiotics at the hands of Locke and his successors. Moreover, the new emphasis on the Hippocratic and Galenic concept of crisis was a significant rhythmological event because this concept was, as we will see, eventually transferred from medicine to economy by Clément Juglar. The concept of crisis, as a possibly destructive as much as relieving event was then integrated into the web of concepts related to rhythm, while being considered as periodic, which was not the case in medicine.
Another important contribution to the qualitative and semiotic approach to the pulse was that of Théophile de Bordeu (1722-1776) who was physician to the Countess du Barry and a close friend of Diderot. In his Recherches sur le Pouls par rapport aux crises – Investigations on Pulse in Relation with Crises published in 1756, he used Solano’s prognosis work and crossed it with the diagnosis theory of organic pulses of Galen and even the Chinese. Changes in the pulse, particularly in its rhythm, were not only announcing future crises, but they were also indicating the state of the organs. Rhythms were signs of particular disturbances in the “animal economy.”
Driven by his semiotic search for signs, Bordeu developed new diagnosis technique. Pulse recognition depended not only on the tactile abilities of the physician but also on his skills in auditory perception. Physicians were required to memorize various acoustical patterns, then match them to the “live” pulse pattern of the patient perceived during observation. The introduction of sound in medicine, which had hitherto been concerned mainly with sight and touch, opened up entirely new clinical practices that were eventually to become the basis of modern auscultation (for more details see Sykes, 2012 and 2015).
The debate between Mechanistic and Semiotic pulse theories is perfectly staged in the article “Pulse” written by Jean-Joseph Menuret de Chambaud (1739-1815) in Diderot’s and d’Alembert’s Encyclopédie (1765, vol. 13, p. 205-240).
I reproduce in this paragraph a part of the enlightening biography established by Kafker & Kafker (1988). Menuret got the doctorate in medicine in 1757 at the Montpellier Faculty of Medicine. Some time afterwards he continued his medical investigations in Paris, where he worked with Théophile de Bordeu and studied chemistry with Guillaume-François Rouelle. Menuret was recruited for the Encyclopédie by one of Rouelle’s disciples, Venel, who was unable to manage all his commitments to the work. Strongly influenced by Bordeu, Menuret championed in his articles many of the leading ideas of the Vitalist school of Montpellier; he challenged the Mechanism of Hermann Boerhaave, the Animism of Georg Ernst Stahl, and the Chemical theories of Thomas Willis. However, in the article “Influence ou influx des astres,” he wrote of the moon’s and sun’s effects on health.
In his article, Menuret presented one after the other the Ancient Herophilean-Galenic pulse lore; the new Mechanistic conception of pulse; Marquet’s and Bordeu’s most recent contributions; finally, the Chinese pulse lore as it had been recently discovered by missionaries.
Menuret’s opinion was very close to Bordeu’s. He criticized the exaggerate importance given to Harvey’s discovery, the disinterest of the Mechanicist physicians for the pulse as “sign,” the abstract debate about its “strength and causes,” and contrasted it with an attention to its variations and their “significations.” As for Bordeu, the Chinese had developed a full semiotic theory concerning the pulse that was worth inquiring because it was close, in spirit if not in fact, to that of the Vitalist school.
Bellini is one of the first and most famous authors who considered the pulse mechanically. Hoffman followed his system and claimed to prove, in a particular dissertation, that the pulse must be subject to the rules of mechanics. Boerhaave and all his followers, all the physicians who have embraced the common theory [la théorie vulgaire], based on the ill-conceived and too generalized famous blood circulation, and on the insufficient laws of inorganic mechanics; all these physicians, I say, who are still the most numerous and almost dominant in the schools, have adopted their opinions on the pulse. They make little use of this sign, examine it without attention, and draw little and very uncertain knowledge from it. But on the other hand they make it an important object of their dissertations, their arguments and their calculations. They submit it to mathematical analysis, and are much more concerned in determining geometrically its strength and causes, than in correctly grasping its differences, and in estimating their meanings. (Menuret de Chambaud. “Pouls,” Encyclopédie, 1765, vol. 13, p. 215, my trans.)
Bordeu was followed in 1767 by Henri Fouquet (1727-1806) who published in 1767 his Essai sur le Pouls, par rapport aux affections des principaux organes, avec des figures qui représentent les caractères du Pouls, dans ces affections – Essay on Pulse in Relation with the Affections of the Main Organs, with Figures Representing the Characters of the Pulse in these Affections. Fouquet combined Solano’s critical pulses and Bordeu’s organic pulses and illustrated them with drawings. He too was committed to touch and hearing, and rejected both Marquet’s musical notation and Mechanistic pulse rating, which he ironically called mere “pretense,” “sphygmometers”—a name that was to become very successful in the 19th century—and “small physical curiosities.” Semiotics was much more useful to medicine than arithmetics and physics.
It may be judged now, by all that has hitherto been said of the true and intrinsic character of the pulse of the organs, of the importance which must be given to the system of Herophilus, which pretends to subject the rhythms of the pulse to the rules of music, and other similar systems advanced by some Modern [Marquet’s New Method was explicitly cited].
Finally, one can draw from it some esteem for these sphygmometers [sic] and all these other small physical curiosities, with which the Mechanicists have entertained for so long the rational medicine, although they could not embarrass/thwart [embarrasser] with it the practical medicine. (Fouquet, Essai sur le pouls..., ed. 1818, p.77, my trans.)
At the beginning of the 19th century, René Laennec revolutionized diagnosis by introducing the stethoscope and auscultation. In 1819, he published a long treatise De l’auscultation médiate ou traité du diagnostic des maladies des poumons et du cœur, fondé principalement sur ce nouveau moyen d’exploration – On Mediated Auscultation or Treatise on the Diagnosis of Lungs and Heart Diseases Mainly Based on this New Exploration Means, where he emphasized the need for a thourough observation of the heart rhythm.
595. The motions of the heart must be examined in four principal respects: 1. the extent to which they can be heard by means of the cylinder [the stethoscope]; 2. the shock or impulse strength of the organ; 3. the nature and intensity of the sound that it makes; 4. the rhythm according to which its various parts contract. (Laennec, De l’auscultation médiate..., vol. 2, p. 196, my trans.)
Laennec defined rhythm as the order and ratio between “the contractions of the various parts of the heart,” i.e. not any longer between the motions of the arteries but still as ratio and order.
635. By rhythm I mean the order of the contractions of the various parts of the heart as they are heard and felt by the cylinder, their respective duration, their succession, and, in general, their relation to each other. (Laennec, De l’auscultation médiate..., vol. 2, p. 215-216, my trans.)
According to his findings, this order was composed of three successive, dissimilar and periodic motions: first, the contraction of the auricles for a quarter of the full cycle; then a rest for another quarter; finally, the contraction of the ventricles for the remaining half.
640. The duration of the contractions of the auricles and ventricles seems to be determined more or less in the following manner. In the total duration of the time in which the successive contractions of the various parts of the heart are performed, a third or more, or even a quarter, is used by the systole of the auricles; a quarter, or a little less, by absolute rest, and half or so by systole of ventricles. (Laennec, De l’auscultation médiate..., vol. 2, p. 218, my trans.)
Healthy men enjoyed a “regular rhythm” even if the latter could vary or be disturbed in many ways.
I will, consequently, describe in their successive order the phenomena which the heartbeat of a healthy man provoke in the ear, a man whose heart has the most favorable proportions for the free exercise of all functions. (Laennec, De l’auscultation médiate..., vol. 2, p. 216, my trans.)
653 [...] In many circumstances, which are not always illnesses or even serious ailments, this rhythm is subject to various anomalies: physicians ordinarily reduce them to three principal species, palpitations, irregularities, and intermittency. (Laennec, De l’auscultation médiate..., vol. 2, p. 226, my trans.)
In Laennec’s vocabulary, rhythm was still different from beat and frequency.
On May 22, the symptoms were still the same, without increase or decrease. The face was continuously red, the skin moist, the pulse quite natural, either in terms of frequency, or of development and rhythm. (Laennec, De l’auscultation médiate..., vol. 2, p. 413, my trans.)
Tracing the pulse – Rhythm as Wave (from Hales to Ewart – 1733-1894)
Qualitative and quantitative methods for measuring the pulse were not to remain definitively at odds though. Substantial progresses were made in mathematics, fluid mechanics and measuring devices which enabled the two methods to merge.
The mathematical language in which Nature’s book was written, as Galileo put it, rapidly became very sophisticated. As soon as the end of the 17th century—between 1684 and 1704—Newton and Leibniz, resuming without knowing it with some ancient rhuthmic Archimedean concepts (see, vol. 1, chap. 5), published essays which leaped from geometry, the study of shape, and algebra, the study of the generalizations of arithmetic operations, to calculus and the study of continuous change and variation.
Then fluid mechanics could penetrate physiology. In his famous treatise on the circulation of blood, Harvey had applied the laws of mechanics to the circulation of blood in arteries and veins, which was considered as that of any other liquid, varying in consistency and circulating under varying pressure in various kinds of pipes. The heart was only a pump and the pulse the result of the blood being propelled under a certain pressure and with a certain velocity into the arteries then in the veins. But Harvey still lacked mathematical instruments to give a full account of the blood dynamics.
The first studies on arterial haemodynamics were developed by Stephen Hales (1677-1746) in a series of papers entitled Statical Essays: containing Haemastaticks (1733). In Experiment 3, for instance, he discussed the velocity at which blood was ejected from the heart of a 10-year-old mare and how it was altered by the elasticity of the arteries.
The systole of the ventricle during which that quantity of blood is propelled, being estimated to be done in one third of the space of time between each pulse, the velocity of the blood during each systole will be thrice as much, at the rate of 5211 feet, that is, 0.98 of a mile in an hour, or 86.85 feet in a minute. Now this velocity is only the velocity of the blood at its first entering into the aorta, in the time of the systole; in consequence of which the blood in the arteries, being forcibly propelled forward, with an accelerated impetus, thereby dilates the canal of the arteries, which begin again to contract at the instant the systole ceases: by which curious artifice of nature, the blood is carried on in the finer capillaries, with an almost even tenor of velocity, in the same manner as the spouting water of some fire-engines, is contrived to flow with a more even velocity, notwithstanding the alternate systoles and diastoles of the rising and falling embolus or force. (Hales, Statical Essays: containing Haemastaticks, 1733, quoted by Parker, 2009)
In 1755 Leonhard Euler (1707-1783) submitted an essay Principia pro motu sanguinis per arterias determinando – On the Flow of Blood in the Arteries as an entry in a prize competition set by the Academy of Sciences in Dijon. For this paragraph and the next, I used Parker (2009) and Tijsseling & Anderson (2008). In it he set out the one-dimensional equations of conservation of mass and momentum in a distensible tube. In his notation
1.
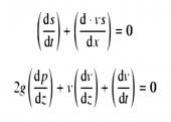
2.
where s is the cross-sectional area, v is the average velocity, p is pressure, g is the density of blood, t is time and z is the axial distance. However, he was quite unsuccessful in proposing a formula that could simply show the relationship between the mechanical forces and the dynamic measures of the arterial pulse wave. He posited some rather unrealistic constitutive laws (tube laws) for arteries and unsuccessfully tried to solve the equations as he had done for rigid tubes by reducing them to a single equation that could be solved by integration (Parker, 2009).
In 1808, Thomas Young (1773-1829) published a paper entitled “Hydraulic Investigations, subservient to an intended Croonian Lecture on the Motion of the Blood.” In this paper he established the correct formula for the wave speed in an artery but gave no derivation of it. The celerity (c) of a pressure wave, propagating in an incompressible liquid of mass density ρ, contained in an elastic tube with Young’s modulus E and where e/D is the ratio of wall thickness to tube diameter, was determined as

In short, Hales’, Euler’s and Young’s studies, as well as others of the same type, showed that the pulse was not to be measured only by its frequency and regularity but also by the volume, the pressure, and the speed of the blood waves that circulated in the arteries. But it took again some time before scientists invented devices capable to measure and record those variables.
The first blood pressure measuring device was created in 1834 by Jules Hérisson who called it “Sphygmomètre – Pulse meter,” probably without knowing of Fouquet’s mockery. Hérisson described his new device in a memoir presented to the Institute of France and published in English the very next year: The sphygmometer, an instrument which renders the action of the arteries apparent to the eye; the utility of this instrument in the study of disease, researches on the affections of the heart, and on the proper means of discriminating them considered. This instrument was composed of a graduated glass tube containing mercury with a semiglobular steel ball at one end. By placing the semiglobular end over an artery, the action of the vessel and the force of its impulse could be shown and measured (Ghasemzadeh & Zafari, 2011, p. 6).
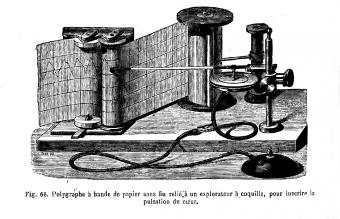
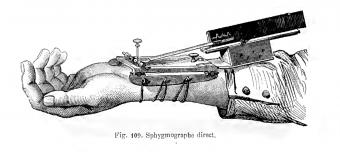
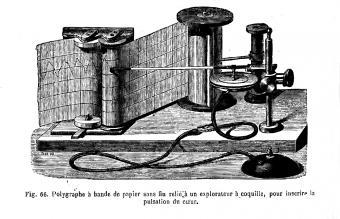
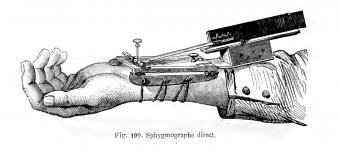
Hérisson’s sphygomètre allowed to measure the arterial pressure but it lacked a recording device. This shortcoming prompted Carl Friedrich Ludwig to create a few years later the Kymograph (1847) or “Wave-writer,” which was a revolving drum wrapped with a sheet of paper on which a stylus moved back and forth recording perceived changes of pressure. Karl von Vierordt adapted it to the measure of the pulse and created the Sphymograph in 1854 which was further improved by Etienne-Jules Marey in 1859.
As a result of the progress made in calculus, physiology of blood circulation, and measure and record technology, the pulse began to be assimilated to a wave in two manners:
First, the blood circulated in the arteries under the pressure of successive waves.
The heart contracts: thereby a wave of increased pressure is set up in the arterial stream; this we call the pulse-wave. (W.M. Ewart, The Pulse Sensations: A Study in Tactile Sphygmology, 1894, p. 18)
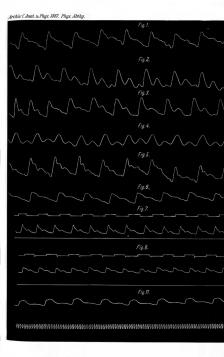
Second—and this was to prove more significant in term of conceptual change—the measures of the volume, the pressure, or the speed of the blood in the heart or the arteries were translated by the recording devices into oscillating curves which motivated Ludwig to call his invention the Kymograph or Wave-writer.
In 1863, Marey published a long study on blood circulation which recapitulated his findings made with the Sphygmographe: Physiologie médicale de la circulation du sang, basée sur l’étude graphique des mouvements du cœur et du pouls artériel avec application aux maladies de l’appareil circulatoire – Medical Physiology of Blood Circulation. Very soon the studies in haemodynamics multiplied. In 1875, William Broadbent (1835-1907) published in The Lancet “A clinical lecture on the pulse: its diagnostic, prognostic and therapeutic indications” (vol. 106, no 2717, p. 441-443). Starting from 1880 there was a wave of detailed studies on haemodynamics. Marey published La circulation du sang à l’état physiologique et dans les maladies – Blood Circulation in Physiological State and in Diseases in 1881 and Broadbent his famous essay The Pulse in 1890.
In all those texts, one can observe a new change in the meaning of the term rhythm as used by physicians. Whereas it had meant for centuries ratio between durations, then little by little beat and frequency, it now denoted the succession of the blood waves shown to the readers by spectacular figures.
In 1863, Marey explained what he was aiming at when creating the Sphygmographe. After mentioning the measure of “frequency,” “regularity,” and “intensity,” which were already regular features in medical pulse rating, he stressed with italics the “specific form” of the pulsations of an artery.
The goal we have pursued in the construction of our Sphygmograph is: to record the pulsations of an artery, not only with their frequency, regularity and relative intensity, but with the specific form of each one of them. (Etienne-Jules Marey, Physiologie médicale..., p. 183, my trans.)
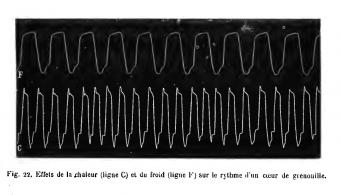
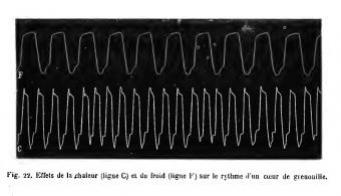
His books and those of his colleagues were full of figures representing the pulse wave of various animals and human beings of different gender, age and health state, under various conditions such as heat, cold, pressure, psychological stress, toxic substances, etc. Figure 22 in La Circulation du sang, for instance, presented the readers with “the effects of heat (line C) and cold (line F) on the rhythm of a frog heart.”
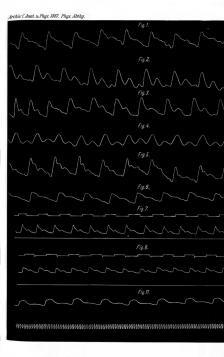
In Germany, important research activities were developed by physiologists such as Johannes von Kries (1853-1928), who published in 1887 an important essay on the “Wellenbewegung des Blutes – blood wave movement” and where one could find the same kind of graphics representing the pulse wave in different parts of the limbs (thigh, arm, in different times of the day).
A thorough study of Marey’s uses of the term rhythm in his 1881 book on pulse shows that he took rhythm first as synonymous with recurring beat, as it had become customary in his time, but also, with succession of graphic waves—as in the previous figures—and by a kind of metonymy, with the very frequency and regularity of these beats and waves which, properly speaking, were only two of their characteristics.
One sees, for instance, the invasive importance given to frequency from the way Marey clarified an expression such as “disturbance of the [heart] rhythm” by phrases like “acceleration,” “slowdown,” and “complete stop of its beats.”
Often, by detaching the heart of an animal and by moistening it with a toxic solution, one observes a disturbance in its rhythm [un trouble de son rythme], a slowing down or an acceleration, and finally a complete stop of its beats [un arrêt complet de ses battements]. (Etienne-Jules Marey, La circulation du sang..., p. 492, my trans.)
Marey’s implicit equating of rhythm to frequency particularly showed through the recurrence of phrases like “acceleration of the rhythm,” which kept returning under his pen (p. 33, 45, 46, 47, 48, 50, 56, 59, 60, 61, 64, 284, 332, 337, 338, 340, 344, 403, 473, 478 n. 1, 484, 487, 488, 493, 597) or the opposite “slowdown of the rhythm” (p. 29, 48, 186, 340, 364, 399, 404, 468, 470, 472, 478, 482, 514). In passing, he also mentioned the “slowdown of respiratory rhythm” (p. 461).
The assimilation of rhythm to regularity was also implicit in Marey’s frequent use of the phrase “regularity of the rhythm” and, even more frequently, “irregularity of (or in) the rhythm” (p. 155, 156, 292, 462, 463, 554, 621, 622, 668, 689, 690).
In both cases, these uses were so frequent that the term that was supposed to be qualified (rhythm) was, so to say, contaminated by and made equivalent with that that was qualifying it (frequency or regularity). As a matter of fact, Marey, sometimes, significantly used phrases such as “acceleration of the heart frequency” (p. 78) or “acceleration of the heart beat” (p. 336), instead of the expected “acceleration of the rhythm,” as if the terms “rhythm,” “frequency,” and “beat” were interchangeable. He also coined, by swaping “rhythm” and “irregularity,” remarkable new phrases such as “the periodic irregularity of the rhythm” (p. 222, 294, 621), “the rhythm of the irregularity” (p. 723) or, in the very last page of the book, “the rhythmic irregularities which are so frequent in old people” (p. 724 – according to a phenomena already described by Galen in De pulsibus ad Tirones, 6). Irregularity itself could be periodic or rhythmic, i.e. regular. Rhythm was then equated with regularity.
In old age patients, irregularities in the rhythm of the heartbeat sometimes occur [...]. In some cases, the irregularity is not complete, because one observes the return, from time to time, of groups of pulsations which are unequal between them, but which reproduce the same rhythm in a periodic way [le même rhythme de façon périodique]. [...] Figure 127 was collected from an old man in whom we observed the following rhythm [le rhythme suivant]. A suspension of the heartbeat [des battements du cœur] was followed by three ordinary pulsations, then a small pulsation after which a normal beat [un battement normal] returned. A new suspension occurred, and so on indefinitely. These periodic irregularities often change several times in a day; one sometimes observe their appearance and disappearance at very short intervals. (Etienne-Jules Marey, Physiologie médicale..., p. 420, my trans.)
In the first chapter of his large essay The Pulse. Illustrated with 59 Sphygmographic Tracings (1882), Broadbent commented the conceptual change that had occurred from Antiquity to Modern Times. The list of pulse differentiae he attributed to Herophilus was not completely accurate—he swapped frequency with speed (see vol. 1, chap. 4)—but he was correct in stressing the fact that rhythm did not mean for Herophilus “the regularity or frequency of the beats” as it was now the case.
[Herophilus] described four qualities in the pulse, size, frequency, force, and rhythm, and gave special attention to the rhythm of the arterial pulsation, by which was meant the relative duration of the wave and the interval, not the regularity or frequency of the beats. (W. Broadbent, The Pulse, 1882, p. 4)
However, his own conception of rhythm was not as advanced as that of the German or the French. In chapter 2, Broadbent described “The Action of the Heart” under three entries: “1. Frequency. […] 2. Rhythm. [...] 3. Force.” Rhythm was clearly assimilated to regularity but it was also strikingly differentiated from frequency.
2. Rhythm.—The rhythm, as well as the rate, of the pulse is determined by the heart, and the pulse, generally speaking, is regular or irregular according as the action of the heart is regular or irregular. The pulse, however, may be made irregular when the heart is acting regularly by beats failing to reach the wrist, and irregularity of the heart’s action may be greatly exaggerated in the pulse. (W. Broadbent, The Pulse, 1882, p. 23)
These assimilation between rhythm and regularity and differenciation between rhythm and frequency were again presupposed a little further down.
A complete account of the pulse, then, should specify (1) the frequency: that is, the number of beats per minute, with a note of any irregularity or intermission or instability of the rhythm ; (2) the size of the vessel [...]. (W. Broadbent, The Pulse, 1882, p. 44-45)
However Broadbent was aware of the semantic shift of the term “rhythm” and thought necessary to make himself clear. In this particular instance, he referred to the “strict sense” as denoting a time-relation between the sound of beats, and “not the regularity of the succession of heart-beats.”
The term rhythm is here employed in its strict sense, as denoting the time-relations of the first and second sounds of individual beats, and not the regularity of the succession of heart-beats. (W. Broadbent, The Pulse, 1882, p. 63)
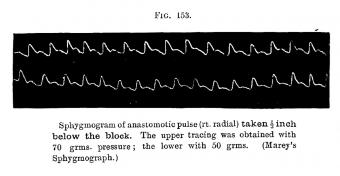
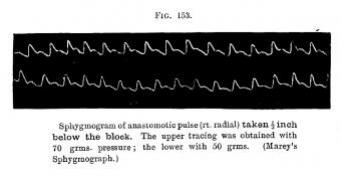
At the end of the 19th century, William Ewart, an English physician with a French education (1848-1929), wrote an interesting book entitled The Pulse-Sensations: A Study in Tactile Sphygmology (1894), where he intended to overcome “the relative neglect of a valuable clinical method” which resulted from “the contrast between the mechanical accuracy and elaborate detail of the sphygmogram, and the vague and inconclusive character of the pulse impressions hitherto gained by palpation” (Preface – p. vii). Ewart, who was attached to the qualitative measure of the pulse, was well aware of the effect of the mechanization of the pulse measure and record on “our mental ideation.” He noticed that, in his time, pulse rhythm had become almost identical with pulse wave.
The sphygmogram is indeed the only graphic representation of the arterial-pulse in clinical use, and from it is at present evolved our visual, and in most cases probably also our mental ideation in connection with the pulse-wave. (W.M. Ewart, The Pulse Sensations: A Study in Tactile Sphygmology, 1894, p. 12)
To prove his case, Ewart provided a number of those sphygmograms, some of them taken in Kries’ and Marey’s books.
Although it was not a direct shift and the semantic evolutions have been quite intricate, the medical concept of rhythm underwent between the 16th and the 19th centuries a spectacular transformation. Whereas it was first conceived as a succession of time-lengths organized according to rational proportions and related with the circuits of the heavenly bodies, it was finally defined as a succession of beats or pressure waves, characterized by its frequency and regularity. Medicine adapted the old Platonic-Aristotelian concept based on the Ancient poetic and musical metric to a more Modern metric model based on continuous repetitive variations devoid of metaphysical background.
This does not mean though that the old meanings were entirely replaced by newer ones. What happened was more like a multiplication and superposition of the different senses of the term rhythm. As the case of Broadbent showed us quite clearly, ancient ones were not forgotten and could at times re-emerge in particular occasions.